Laparoscopic Cholecystectomy
Patient’s information
How the Gallbladder and bile ducts work:
The gall bladder a small pouch that stores bile. Bile a green-colored fluid produced by the liver cells. It collected within the bile ducts and transported to the gall bladder for storage. The bile from the liver mixes up with the food from the stomach and helps to absorb vitamins (like vitamin D and E) and is required for the process of breaking down fats from our diet.
The presence of food within the first part of the small intestine (duodenum) stimulates the gall bladder to contract and squeeze bile out of the gall bladder, into the duodenum. Here it helps to digest and absorb the fats in the food.
Bile contains bile salts and bile pigments, most of which recycled and the excessive ones passed out of the body through urine and feces. The blockage of the bile duct system leads to dark urine and pale stools.

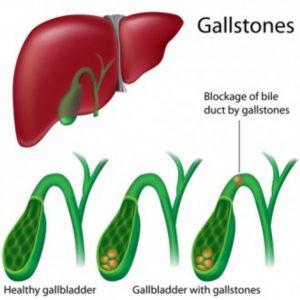
Gallstones:
The gallbladder a pear-shaped organ, attached to the underside of the liver in the upper right side of the abdomen. It stores the bile, which produced in the liver and released through the common bile duct, to aid the digestion of fatty foods.
Gallstones form when certain chemicals in the bile solidify. Gallstones are very common and do not always cause problems, but if they block the exit from the gallbladder they can result in severe pain, nausea and vomiting, and local inflammation. Occasionally stones pass into the bile duct where they can cause jaundice and sometimes acute pancreatitis, both of which can be life-threatening. Avoiding jaundice and pancreatitis is the most important aim of gallstone treatment.
laparoscopic cholecystectomy:
Before the 1990s the gallbladder was almost always removed through an incision several inches long. Laparoscopic surgery allows the same procedure to be carried out using a number of smaller incisions (as shown in the figure), causing you less discomfort after surgery, which therefore allows a faster return to normal activities. A telescope is inserted through the main incision at the umbilicus (tummy button), which usually gives a very good view of the gallbladder.

More about laparoscopic cholecystectomy:
An x-ray sometimes taken during the operation to identify whether any stones have entered the bile duct. If so, they removed during the operation or by a separate endoscopic procedure performed after recovery from the cholecystectomy. After securing the duct and blood vessel which connect the gallbladder to the bile duct and the main artery to the liver, the gallbladder freed from the liver. It then removed from the abdomen through the largest of the incisions.
Alternatives to surgery:
Once formed, gallstones do not disappear spontaneously, and treatments to dissolve them ineffective. Bile duct stones can be treated by an endoscopic procedure, but only surgical removal of the gallbladder is effective for stones in the gallbladder itself. Removal of the gallbladder does not cause any postoperative digestive problems.
After cholecystectomy you can expect to have an IV infusion in place from theatre. This removed once you start drinking. On some occasions it may be necessary to stay longer than a day case patient and stay overnight in hospital.
Wound care:
The surgical incisions are sometimes closed with metal clips which are easily removed after around 10 days. Alternatively, dissolvable stiches may be used. Small dressings applied over the clips can be replaced if they fall off, or become loose after bathing or showering. It best not to soak the wounds for too long in the first few days after surgery. If dressings are in place following surgery extra dressings will be supplied on discharge.
Drains:
A small plastic tube sometimes left in the space where the gallbladder was, in order to drain away any fluid from the operation site. Occasionally some bile may leak from small ducts close to the gallbladder and the drain can prevent accumulation of bile, allowing healing to occur. In most cases the drain removed before discharge from the hospital. If you have had the procedure done as a day case, then the drain should be removed within three hours.
Some pain or discomfort to be expected following any type of surgery. You may be given painkillers while on the unit and some to take home. You may experience some shoulder tip pain, caused by trapped gas from the operation. This will gradually diminish by sucking strong peppermints. You may also find gently walking around helps to relieve the discomfort.
Diet:
You will be allowed fluids immediately after surgery and food once you able to tolerate it.
Nausea/vomiting after surgery: You may feel sickly but this should not stop you from eating and drinking.
Exercise: You will be encouraged to get out of bed soon after surgery and to mobilise as soon as possible.
Driving:
Do not drive for 24 – 48 hours following your anaesthetic. After this time you may drive when it feels completely comfortable for you to do so and you are able to perform an emergency stop comfortably.
Work: It is advisable to have at least 1- 2 weeks off work. You may return to work when you can perform your job comfortably and safely. The staff can provide you with a doctor’s certificate to cover time off work if required.
Day case patients:
If you have had this procedure done on the day surgery unit then you can expect your stay to be at least 4-6 hours. To provide privacy and dignity to all patients, relatives/carers are not allowed in the recovery area. You will need to have a responsible adult with you for the first 24 hours after your surgery.
Further appointments:
There usually no need for you to come back to the hospital after gallbladder surgery unless other procedures are required for stones in the bile duct.
Potential complications:
All intra-abdominal operations regarded as major surgery and carry some risk. The main specific complications of cholecystectomy are injury to the bile ducts, blood vessels, and bowel immediately adjacent to the gallbladder. These injuries are rare but can require further major procedures for their correction. If the gallbladder is very inflamed, it may be safest to convert the laparoscopic operation to an ‘open’ cholecystectomy through a larger incision. This requires a longer postoperative stay and a slower return to full activity but still gives excellent long term results.
If you have any further questions or worries please feel free to ask the staff on your ward, your surgical team or your clinical nurse specialist.
Patient Help Line (PHL) a service that offers support, information and assistance to patients, relatives and visitors. They can also provide help and advice if you have a concerns.
The PHL office is located on the ground 6th floor of the “Quaid e Azam International Hospital”, Islamabad our staff will be happy to help and assist you.
Transplant coordinator:
Mr. Touseef Ahmed 0333-1027353
Transplant Coordinator: (for post-transplant follow up patients):
M. Zaheen Hashmi 0333-1027354
Hepatobiliary & Pancreatic Surgery Services:
Muhammad Asif 0341-0543883
24 Hours Patients emergency Helpline: 0333-1027356
Email: info@faisaldar.com
Counselling service: The counselling service offers free and confidential sessions to our inpatients, outpatients, their relatives and friends. If you would like to meet with one our counsellors you can contact us on 0333-1027356
Transplant coordinator:
Mr. Touseef Ahmed
0341 0543883
0307 5446668
Opd appointments
042 111 117 554
042 36093000
Email: info@faisaldar.com